Case Study - Diagnosis and Treatment using PODOSmart
- Sales Team
- Canonbury
- 7 Oct 2020 views

Presentation
Presented to the clinic via consultant foot and ankle surgeon complaining of right sided lesser metatarsal pain. Plain radiographs demonstrated positive healing with good callus formation and remodelling, she was placed on structured training approach with focus on the swimming and cycling aspects of her training schedule. Patient was subjected to DEXA scan which revealed mild osteopenia, this was being actively treated and her blood tests were normal including Vitamin D. The decision was made to treat non-operatively.
History
Patient has been a competitive athlete all her life, she has competed in kickboxing, fell running, cycling and swimming. Essentially decided to combine the sports (aside from kicking people) and divert all her attention to Tri-Athlon. This has culminated in Iron-Man training for the past two years and successful inclusion into the Iron-Man Team GB age group for full and half distance. Patient works for pharmaceutical company and mixes office work with mobile tasks.
Assessment
Patient was advised, prior to my consultation, on hard soled footwear and opted for carbon fibre based approach. This further exacerbated the issue and essentially provoked her second fracture; the third metatarsal was the initial pathology, the clinical inclination was then mechanical overload due to antalgic gait, further loaded the adjacent second metatarsal resulting in increase tissue stress and eventual stress response. From clinical experience working with highly competitive athletes for many years, there is definitely no “one size” fits all approach with regard to structural orthotic support. In this case, the functional outcome measures with regard to foot function and medial column facilitation did not warrant a high density support. There was no leg length difference and she demonstrated excellent muscle symmetry, excellent posterior chain recruitment and activation through out the gluteals and good, powerful quad complex activation and strength.
Initial Gait assessment using the Podosmart technology approach combined with clinical assessment demonstrated good loading patterns but there was an increase in load response at propulsion on
the right side of 12% (unfortunately I do not have the stills to prove this). Based on clinical opinion and history taking, the clinician felt this was more a lack of loading as opposed to a direct cause of overloading and a reluctance on the part of the athlete to load dynamically.
Treatment
Opted against orthotics and instead a combined approach of soft tissue work, myofascial release and a specialist Gait retraining programme was issued to provoke the athlete into loading the foot equally during a run. She was then reviewed at 6 weeks to determine if the response had changed.
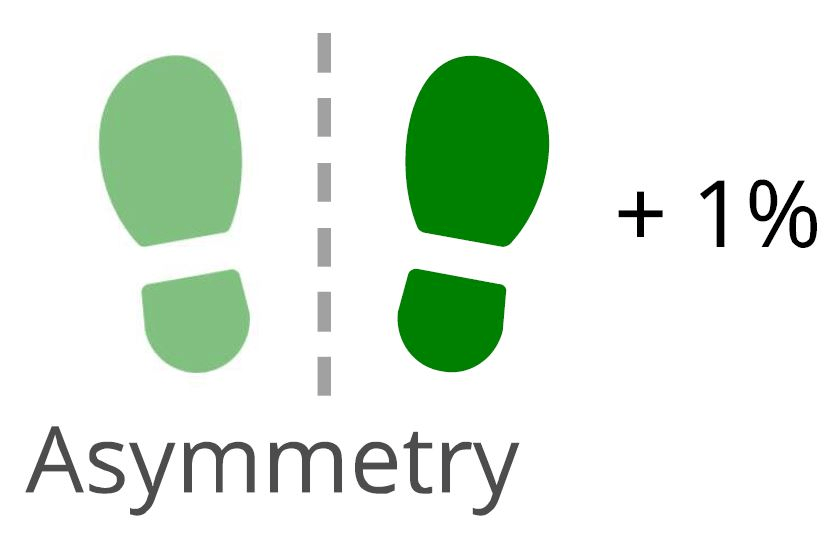
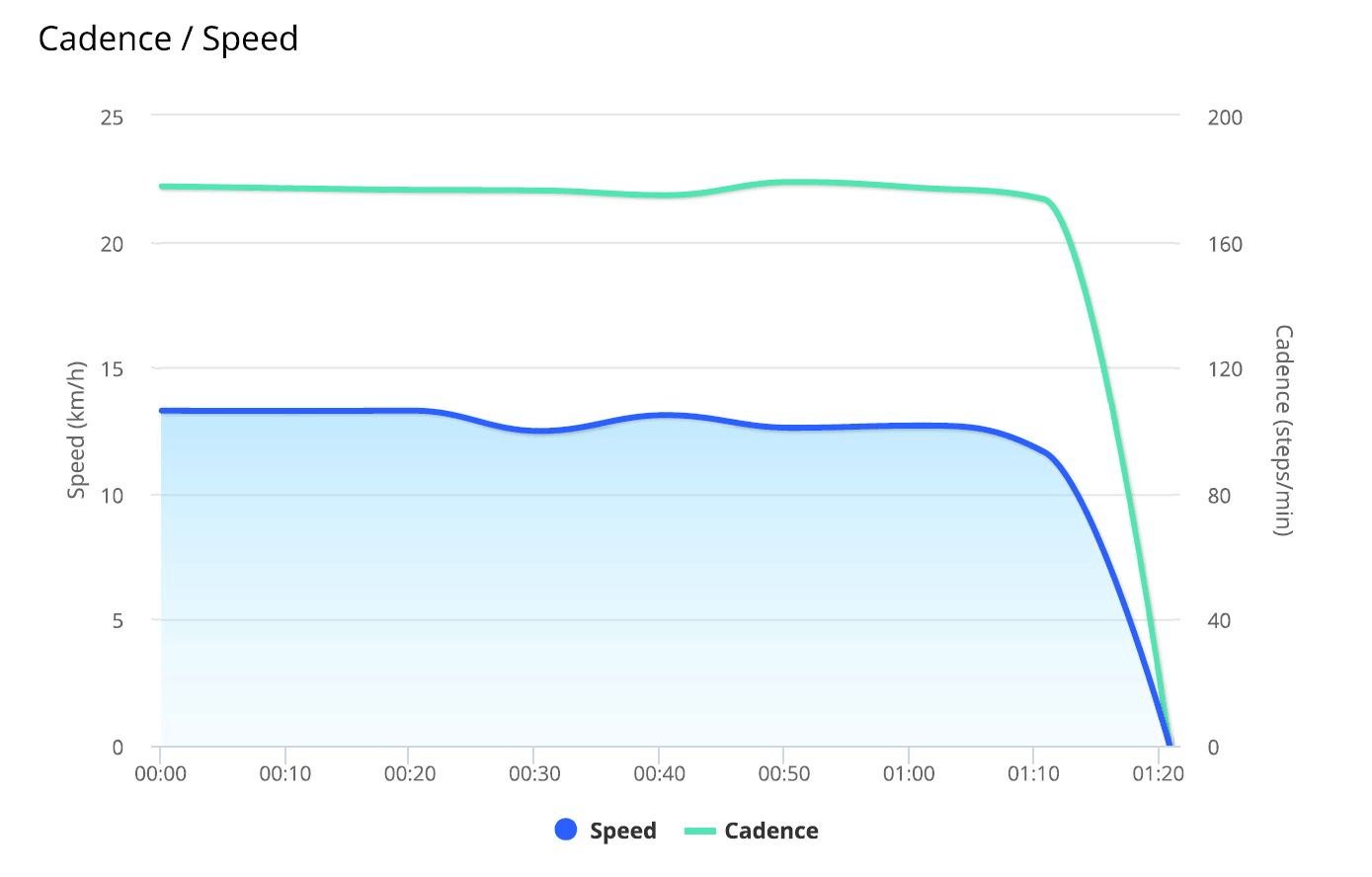
Review
A repeat Podosmart analysis was carried out at week 6. This provided excellent feedback with the loading reducing from 12% to 1% (see below); an excellent clinical outcome and a very happy athlete. On further scrutiny of the results, we established that there was a reluctance to let the forefoot load compared to the contralateral and clinical assessment demonstrated soft tissue hypertonicity in the calf on the right side, in particular the medial gastrocnemius and muscular tendinous junction. It is important to point out that 1% differential is acceptable, but given the competitive nature the approach was simple in order to combat the final 1%. Combined shockwave/Graston Technique and deep tissue massage to free up the calf and allow the foot to plantar flex and education to the athlete on the limitation; utilising the Podosmart images and findings helped her visualise her goals and focus her training.

Conclusion
Essentially using the Podosmart combined with clinical expertise allowed successful treatment of an athlete without the need for over prescribing orthotics. The technology helped identify specific parameters for treatment and help the athlete understand her problem which in any clinical scenario is fundamental. Patient education and participation should be paramount.
Posts